Policy Shifts Against The mRNA Platform Rapidly Emerged This Past Week

OHIO STATE UNIVERSITY WEXNER MEDICAL CENTER
This week a nurse reached out with disturbing descriptions of some major changes she has witnessed inside the Ohio State University Medical Center (OSUMC) system.
OSUMC s a large and comprehensive healthcare organization, with a significant presence in Ohio and a strong focus on research, education, and patient care. It is a massive institution with over 23,000 employees, including:
-
Over 2,000 physicians
-
More than 1,000 residents and fellows
-
Nearly 5,000 nurses
Lets start off with this screenshot of a webpage from OSUMC’s website which provides information to the public as to where they can get Covid-19 vaccines. Check out the highlighted sentence at the bottom of the page:
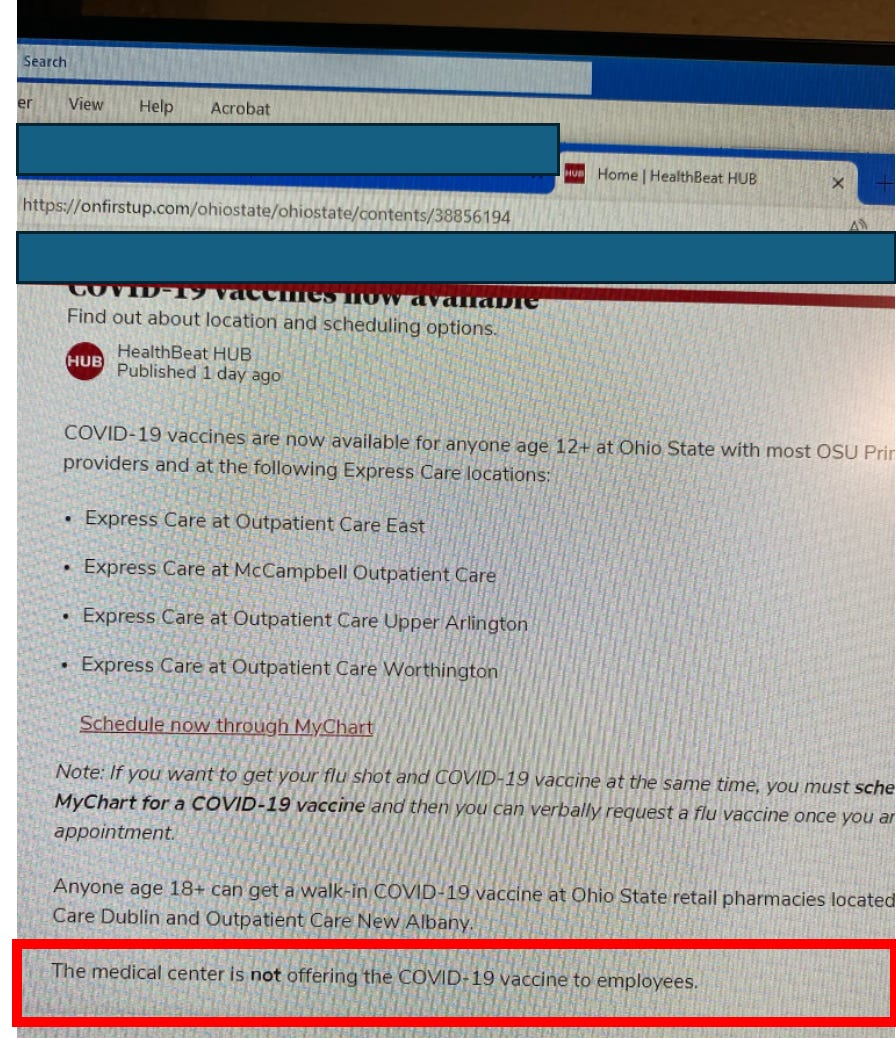
Wait, what? Ohio State is suddenly no longer offering the Covid-19 vaccine to any of their employees but they are happily offering to inject them into the public? How can such a policy be justified? Why was this change in policy done and why was it done so quietly?
Let’s get this straight. Ohio State’s leadership is now making an institutional decision that employees should not be offerred access to any Covid-19 mRNA vaccine. I am (pretending to be) confused. I mean, if the vaccines could protect patients from being infected by staff members and they were safe to give to staff members, why wouldn’t you do everything possible (like a mandate) to ensure they receive them?
The only possible reason for the action above is that either OSUMC leadership recently discovered that the vaccines: a) do not work or b) are not safe. I think you would agree that, of the two possible answers, the only one that makes sense to explain this abrupt change in policy is B) they are not safe. I say this because if they were safe but instead just didn’t really work very well, Ohio State would not have the incentive to divorce themselves so abruptly and strongly from the recommendations of our benevolent federal government. I believe such an action would pretty quickly and negatively impact federal research funding by the NIH. It is my belief that agency’s money kept the nations 126 major academic medical centers in line throughout Covid, as those CEO’s and Deans are well aware that NIH retaliation in terms of rejecting grant funding if they “dissent” is real and happens (inflated reimbursements from the gov’t was another one of course).
I asked the brave browser AI, “why is Ohio State Medical Center no longer offering Covid-19 vaccines to its employees?” Two sentences jumped out:
-
“Based on the provided search results, it appears that Ohio State Medical Center did offer COVID-19 vaccines to its employees at one point.”
-
“Without further information or clarification from Ohio State Medical Center, it’s difficult to provide a definitive answer on why they may not be offering COVID-19 vaccines to their employees.”
So it must be the case that Ohio State leadership somehow found themselves a stronger financial disincentive to subjecting employees to Covid-19 vaccine injection. Where would such a disincentive come from? Answer: lawsuits. I also suspect that fear of worsening staff shortages from disability and/or death further disrupting operations played a role as well (as you will learn below).
This new policy action (taken very quietly) is absolutely dam breaking to me in terms of progress towards the truth about the mRNA platform getting out to the public. It is also appears ethically reprehensible, i.e. the institution made the decision to keep jabbing the public with a toxic and lethal vaccine while becoming aware that same vaccine is either exposing them to unmanageable legal risks and/or is disrupting their operations by negatively impacting the health of their workforce. Welcome to dystopia.
Next, lets take a “little deeper look under the hood” as to what is going on at OSUMC. I think, after reading the below, it is not an overstatement to say that their system is altering on many levels. I would not want to be a patient there, solely based on what I learned from this nurse. Sorry not sorry OSUMC.
What follows is a para-phrased summary of a long telephone conversation I had with my newest nurse informer. She describes the beginning of a sea change in both perspective and open discussion around the “vaccines” that has occurred within OSUMC over the past 6 plus months. At the same time, she tempers that reality by later noting that many staff still have no ability to associate these changes to the vaccines (even when themselves have fallen ill). Although I can’t take credit for the start of that change in awareness, it is what I have worked tirelessly toward for the past 3 1/2 years. However, hold on to your hats folks because what is happening in hospitals in regards to the quality of medical care right now is downright disturbing.
Here are the most potent pieces of information I gathered, in no particular order:
-
An increasingly noticeable number of doctors and nurses and staff have “died suddenly,” “died unexpectedly,” or have become disabled and ill from injuries and/or cancer. The youth and health of these employees have been increasingly remarked on amongst staff (not to mention the deluge of previously healthy and/or young patients they are now presenting with severe and/or atypical (for that age) illnesses. Remember, cancer used to largely be a disease of aging.
-
Consequently, the suspected role of the vaccines in most of the deaths is more of an open secret and of growing concern among staff there. To wit, Ohio State University Medical Center (OSUMC) also recently stopped emailing out obituaries of prominent or veteran employees when they die. Why you ask? Because of both the number of them as well as the comments posted by employees that began openly calling out the likelihood that the vaccines were a cause (i.e. they would point out the dates of the decedents vaccination and their death). Unsurprisingly, she also told me OSUMC would quickly censor any posts of that nature (despite containing no foul language, personal attacks, or threats). From a phone conversation we had:
“Yes, this is huge. Lots of internal cases of death and disabilities. They quit posting internal obits for staff. The comments underneath them were showing that people knew why everyone was dropping dead for baffling reasons. So those went away.”
-
A number of physicians (the most noticeable of them being superspecialists who cannot be replaced easily), besides dying, are also leaving due to disability or retiring due to health reasons.
-
She is hearing of a growing number of lawsuits by family members of these physicians against OSUMC for the mandates which led to the deaths or disabilities.
-
One lawsuit was filed by a widow of a physician who dropped dead suddenly. Interestingly, she demanded an autopsy with staining for spike protein and the heart was found “loaded with spike.”
-
Outcomes of organ transplant patients have been plummeting since the mRNA campaign. It got so bad that, in a complete reversal from two years ago where the programs had insisted on both donors and recipients getting jabbed, at OHSUMC they apparently no longer require or recommend mRNA vaccines to recipients and may be prioritizing organs from unvaccinated donors. Whoa. Apparently one of the reasons is that recipients were developing new “systemic” conditions that were not typical or expected in transplant patients previously.
-
Minutes of administrative and policy committee meetings are no longer openly available on the internal OSUMC website and are instead only available if you “sign in” (presumably so they know who is looking up these minutes).
-
When physicians die suddenly, this creates a huge mess operationally due to the fact “open notes” in the electronic medical record (EMR) can’t be closed and the chronic, ongoing care of large numbers of often long time or highly active patients become disrupted. In her words, “dealing with the practice of a doc who died is a mess - dealing with open notes, ongoing patient care, patient calls, and maintaining plans of care.”
-
Many of the disabilities and deaths of physicians were discovered by this nurse while she was following up on notes that were “left open” in the EMR. She would then be told by the staff about the injury, death, or disability of the health care provider who started the note. Many of the illnesses or disabilities were described to her as being due to neurological issues - either overt neurological deficits or cognitive decline/impairment and even dementia (AMD comprehensively compiled the data showing the negative cognitive impacts from the mRNA vaccines here). Further, adding the “abandoned” patient panel to healthier and still working physicians in that specialty was causing further strains.
-
Cancers are exploding, causing massive strain on oncology services. Particularly glioblastomas to the brain as well as to the spine. Also, case managers for the large number of cancer patients were stating they were not retiring due to the patient volume in need.
-
Even worse, cancers are being missed at high rates given that the “index of suspicion” in younger patients is not appropriately high enough. As a result, doctors are missing cancers as evidenced by retrospectively “obvious” signs and symptoms in the record.
-
Applications for both short and long term disability have risen so much they have created backlogs and delays that staff have noticed and are more openly talking about. The often young ages of the staff applying for disability has not gone unnoticed either.
-
She knows of several colleagues either declining or dying from cancer but are forcing themselves to work in order to provide for their family.