Video: Jeremy Elliot - Nothing Disrupts the System Like An Inquisitive Mind
Jeremy Elliot breaks it down perfectly!
Jeremy Elliot perfectly breaks down the massive fraud being perpetrated on all of us!








| Stats |





Jeremy Elliot perfectly breaks down the massive fraud being perpetrated on all of us!
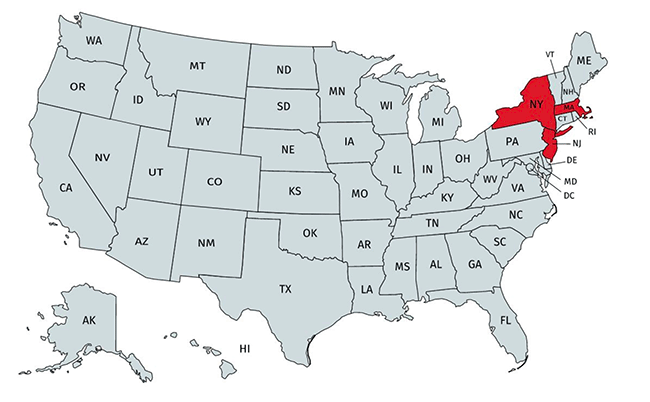
Despite the recent coronavirus alleged surge in southern states, three states—New York, New Jersey, and Massachusetts—account for about 42 percent of COVID-19 deaths in America. Why?
In a recent article in The Atlantic, Thomas Chatterton Williams decried America’s handling of the coronavirus.
The words “utter disaster” are used, and Williams, an expatriate, contrasts America’s response to that of France, where he currently lives.
“As Donald Trump’s America continues to shatter records for daily infections, France, like most other developed nations and even some undeveloped ones, seems to have beat back the virus,” Williams writes.
To be sure, the US response to the coronavirus was far from perfect (more on that later). But the article shows one of the challenges with this pandemic: even as more data is acquired, the picture doesn’t always get clearer.
In some ways, COVID-19 data are like a Rorschach blot from which writers, politicians, and experts can glean whatever conclusions they wish to find. Take Sweden, where daily COVID-19 deaths recently reached zero.
According to Newsweek editorial director Hank Gilman, Sweden’s “lighter touch” approach was a failure because seven times as many people died there than in neighboring Scandnavian countries such as Finland and Norway. He is not alone in the assessment.
On the other hand, Sweden suffered far fewer deaths per capita than several European neighbors that instituted strict lockdowns—including Belgium, Italy, Spain, and the United Kingdom—and has avoided some of the economic fallout other nations have endured. Unlike other countries, its currency is growing stronger.
Indeed, Sweden’s death rate is remarkably close to that of France, which Williams praised as a model in contrast to the “utter disaster” in the US. However, the US actually has a lower per capita death rate than both Sweden and France—at least for now. (While it’s true COVID cases are on the rise again in the US, deaths recently reached three-month lows.)
This raises questions about how we measure success in the age of COVID-19. While most attention is being paid to rising case numbers, death tolls would seem to be the most important metric. While US deaths per capita (401/1M) put the country among the ten highest in the world—ahead of France and Sweden, but just below the Netherlands—those numbers also don’t tell the entire story.
Few may have noticed that 42 percent of all COVID deaths in the US come from just three states—New Jersey, New York, and Massachusetts. These three states account for nearly 56,000 of the nearly 133,000 deaths in the US, even though they represent just 10 percent of the population. If these three states are excluded, the US suddenly finds itself somewhere in between nations such as Luxembourg (176/1M) and Macedonia (166/1M), where some of the better fatality numbers in Europe are found.
3 US states—New York, New Jersey, and Massachusetts—account for roughly 42% of all #COVID19 deaths in America.
— Jon Miltimore (Parler: @Miltimore79) (@miltimore79) July 7, 2020
These same states represent 10% of the US population. pic.twitter.com/AS6DyG3822
Why have New York, New Jersey, and Massachusetts suffered so much more than other US states? We don’t yet know the answer to that question, but evidence suggests it could be policy related.
Texas Doctor Claims Covid Cure as Big Pharma Backed Media Attempts to Cancel Him. Dr. Richard Bartlett’s findings on his experience treating COVID-19 patients with the inhaled steroid budesonide, a drug commonly used to treat asthma.
By Robert F. Kennedy, Jr., Chairman, Children’s Health Defense
ChildrensHealthDefense.org
New documents obtained by Axios and Public Citizen suggest that the National Institute of Health (NIH) owns half the key patent for Moderna’s controversial COVID vaccine and could collect half the royalties. In addition, four NIH scientists have filed their own provisional patent application as co-inventors. Little known NIH regulations let agency scientists collect up to $150,000.00 annually in royalties from vaccines upon which they worked. These rules are recipes for regulatory corruption.
NIH’s stake in the jab may explain why Anthony Fauci moved Moderna’s vaccine to the front of the line and to let Moderna skip animal trials despite the experimental technology and the inherent dangers of Coronavirus vaccines. Every prior coronavirus vaccine has proven problematic and can be lethal to animals due to COVID’s unique penchant for “pathogenic priming.” Death occurs only after a vaccinated animal encounters the wild virus.
Public health advocates and scientists criticized Fauci’s decision to skip animal trials as reckless. It may also explain why Anthony Fauci arranged a $483 million grant to Moderna from a sister NIH agency, BARDA, despite the fact that Moderna has never brought a product to market or gotten approval.

Fauci’s infusion made Moderna CEO Steve Bancel a billionaire and further enriched Fauci’s mentor and co-investor Bill Gates. It may also explain why Fauci publicly announced he was “encouraged” by Moderna’s catastrophic Phase 1 clinical trials despite the fact that 20% of the high dose and 6% of the low dose groups of super healthy volunteers had Grade 3 “severe or medically significant” reactions following vaccination. Those results would have spelled DOA for any other medical product. After getting the abysmal news, Bancel and four other Moderna executives immediately dumped more than $89 million in stock and Fauci was forced to make his optimistic public assessment to save Moderna’s plummeting shares from death spiral.
Fauci painted lipstick on that lame donkey and now he’s trying to convince everyone it’s a thoroughbred. Moderna and NIH began manufacturing the first of 1 billion doses of the deadly vaccine this month. Fauci knows from experience that no matter how dangerous a vaccine, the easy part is convincing people to take it. Pharma, after all, controls the media.

Before you get out the tar and feathers, note that I am a physician with experience in Expensive Care (Intensive Care) – the art of getting people who have both feet on the banana peel well – or spending as much money as possible on high tech expensive resources as possible before they assume room temperature. That’s all done in the Intensive Care Unit, for those of you not familiar with medical humor.
The US is treating the Wuhan Flu as if it is a single disease that has killed so many people that it will kill the rest of us if we open up the economy. They claim that because we are allegedly having a massive spike in new cases, we have to reverse actions to open up our society. At the very least, we have to put masks on everyone.
In other places I’ve discussed how masks do no good and can actually cause harm. Others have discussed how the actual data on mortality and case count are vastly inflated. But this completely misses a couple of very important points.
First, COVID-19 doesn’t kill people.
There. I’ve gone and said it again. There’s a very important reason for this conclusion. If all you get is the Wuhan Flu, you may get a bit sick, but you won’t even need to go to the hospital. You’ll get over it. That’s because you don’t get a “Cytokine Storm.”
In plain English, CS is a different disease process. It’s an uncontrolled release of signaling molecules that engage the immune system at ludicrous speed. A number of different infections can trigger it. An infection is needed before the Storm can start, but the Storm is a different process. Once it’s underway, it drives the train. We know that the risk of dying from CS following COVID-19 in Florida if you are under age 25 is 0.02%, but if you are over 85, it’s 24.5% (FL Dept of Health as of July 6).

That 1,225x difference in risk proves that something else is in play. The infection is necessary, but it’s not sufficient. CS requires something more than just infection such as COVID-19, SARS, or H5N1 flu. In general, age and infirmity are correlated with bad outcomes, but we don’t know in any detail what factor within those categories is needed. What we do know is that the interventions that work don’t have all that much to do with antiviral effects.
Editor's Note: COVID-19 ALERT: Many people say they just can't tell who to believe most of the time. Well, figuring out who is telling you the truth and who is lying to you is actually quite simple. The people lying to you usually provide very little information that isn't "emotionally charged." This is deliberate because when your emotions kick in, when fear kicks in, PANIC ensues bypassing your ability to think clearly. Then those who are lying to you push a sense of urgency to keep you in fear which keeps you cut off from any critical thought. They also work to vigorously suppress and/or censor information other than the so-called "official story". The people telling you the truth, on the other hand, usually provide you with a lot of information that isn't emotionally charged. They typically also provide source material so you can research what they say yourself. People who tell the truth do their very best to reveal as much as possible and put things into a sensible, balanced "unemotionally charged" perspective. They don't inform in order to create as much hysteria as they possibly can. They inform you in order to provide "real understanding."
Dr. Victory is the kind of Doctor who should be advising the President and directing the response to the COVID-19, not the totally corrupt, self-serving evil numbskulls Dr. Fauci/Bill Gates and Co. who have been deliberately misleading the American People into a totally mindless panic to advance their own sick agenda to force their vaccine on everyone. Fire Fauci. Hire Dr. Kelly Victory! We need TRUTH, not MINDLESS HYSTERIA!
The response by governments around the world to COVID-19 eerily mirrors the Amnesty International torture report, where populations are being systematically isolated, deprived of basic life necessities, inflicted by emotional pain, and psychologically weakened.
Editor's Note: THERE IS NO REASON TO BE SO FRIGGIN AFRAID OF THIS. They (Faucci, CDC, WHO, Gates) are not telling you the truth about existing, affordable and effective treatment for this illness. They have been deliberately censoring, LYING about these treatments because they want you to believe you need to chomp at the bit for a GD untested, dangerous vaccine from psychos Dr. Faucci and Billy Gates.
In this video Dr. Brian Procter explains the truth about treating this current virus that's been going around with inexpensive and effective early-stage outpatient care with a hydroxychloroquine regimen.
More and more good, courageous Doctors, Nurses, and healthcare professionals are speaking out about the TRUTH about what has been going on with the manufactured COVID-19 Scam.
Editor's Note: Were you aware this happened just months before the so-called COVID pandemic appeared? Pretty obvious to me this was a meeting to make sure they had everything in place to manage any efforts to expose what they were up to in order to ensure maximum success of pulling this massive con job off.
In this report we take an inside look at Event 201, which took place in NYC on October 18 2019. Event 201 is a high-level pandemic exercise hosted by the Johns Hopkins Center for Health Security in partnership with the World Economic Forum and the Bill and Melinda Gates Foundation.
| You can send a check or money order to: The KTAO Project P.O. Box 1086 Crestone, CO 81131 or donate online: |




| Stats |