The Folly of "New Cases": War, Deception, and the Crux of Covid-19

In June of 1944 Operation Titanic had 10 soldiers of the Allied Air Service parachute over the French countryside along with 500 "ruperts." Ruperts were dummies, fabric stuffed with straw and sand tossed from the airplanes along with the soldiers. They were equipped with incendiary devices so that, upon impact, they ignited, leaving no trace that they were decoys.
It gave the illusion of an invasion far from where the actual invasion was taking place, which was Normandy. The Germans were duly deceived, diverted their resources, and this deception was decisive in making the Normandy invasion ultimately successful.
Intentional deceptions such as this have been part and parcel to warfare for centuries. These deceptions have often been the deciding factor in determining the outcome of battle.
The war against Covid-19 is no exception. Language around Covid-19 is infused with war metaphors. Time Magazine explains to us "Why the U.S. Is Losing the War on COVID-19," while the NYTimes followed up to tell us "How America Lost the War on Covid-19." In this war, as with Vietnam, we have two related "body counts" to help us understand just how badly we are losing to this viral enemy.
The first count is the cumulative deaths caused by Covid-19. The US recently crossed the "grim mile mark" of 200,000 deaths due to the disease. It is a tragic number of deaths, to be sure. But we can also be sure that, as an infectious disease, the cumulative number of deaths will certainly continue to rise into the indefinite future. No one knows what the efficacy will be of any future vaccine, but Dr. Fauci is hoping for at least 75%. In any case, there will always be unfortunate deaths to add to the cumulative death number. All infectious diseases, and in fact all potentially fatal diseases, are the same in this regard.
No one is anticipating complete eradication of Covid-19. This disease is expected to reach a background level, still infectious and occasionally deadly, but not epidemic. Cumulative deaths will continue to rise. The media will surely continue to toll that ominous bell because it carries the gravity of the situation like no other statistic.
The second count used by the media daily is "new cases." These new cases are telling us just how rapidly this virus is disseminating through the population and is used as what we can expect as a surrogate marker for future deaths. Slowing the rise of new cases and squashing any "hotspots" and "outbreaks" of new case clusters is a prime motive behind essentially all social measures, e.g. mask mandates, social distancing, and business closures. For this reason, it is essential that we understand what a new case actually indicates. And to understand that, we first have to examine polymerase chain reaction (PCR), the laboratory technique used to diagnose a case.
PCR: The Basics
PCR is a technique for exponentially multiplying ("amplifying") small pieces of DNA. DNA, recall, is made of a sequence of nucleotides that line up like beads on a string. PCR uses small, synthetic nucleotide strips called "primers" that bind to the target DNA, the piece to be amplified. These primers come in pairs and bind at pre-chosen regions on the target DNA at two locations that are relatively close to each other. The process of PCR is to replicate the strip of DNA between the two bound primers so that one initial copy becomes two. Run it through another cycle and the two copies become four. And so on.
Source: https://users.ugent.be/~avierstr/principles/pcr.html
SARS-CoV-2 is an RNA virus, not a DNA virus. To perform PCR on this virus it first has to be converted from a strand of RNA to a strand of DNA, a process called "reverse transcription." The technique is thus abbreviated rtPCR.
Let's say we don't know if there is any target SARS-CoV-2 DNA in our sample of blood or, with Covid-19 testing, the sample is from a nasal swab. We place the swabbed sample in a solution, then we add the primers to that solution. If there is no target DNA in the sample, then it doesn't bind to anything. Run through 40 cycles and there will still be no "signal" indicating that target DNA got amplified. That test is designated "negative."
On the next sample suppose there is target DNA on the swab and so in the solution. Primers are added and bind to the target. Cycle, cycle, cycle 40 times. The signal appears, indicating that the target DNA was present in the sample all along. That sample has tested positive for Covid-19. Is the person infected with the virus? That is, after all, the important question we need to have answered.
PCR cannot possibly answer that question.
The full infectious genome of SARS-CoV-2 is approximately 30,000 nucleotides in length. If it is cut in half, for example, neither half will be able to carry out an infection. Only the full intact genome can carry out an infection. But when PCR is run, the target it seeks to amplify is not the full length of viral DNA. In fact it is not half or a quarter of the full DNA.
"Expected amplicon sizes of CDC assays are 72 bp, 67 bp,and 72 bp in length by the N1, N2,and N3, respectively." [1].
N1, N2, and N3 indicate three different regions of the N gene, which the CDC picked as targets for PCR. It is noteworthy that the N1 and N2 targets are considered unique to SARS-CoV-2. The N3 target was intentionally picked because it is not unique to SARS-CoV-2, but "was designed to universally detect all currently recognized clade 2 and 3 viruses within the subgenus Sarbecovirus, including SARS-CoV-2, SARS-CoV, and bat- and civet-SARS–like CoVs." [2]
Amplicon sizes of 72, 67, and 72 tells us that, when PCR is run according to CDC specifications, the three target DNA sequences are 72 nucleotides ("base pairs;" bp), 67 nucleotides, and 72 nucleotides. In other words, each target represents approximately 0.2% of the full viral genome, and adding up all three targets still represents just 0.7% of the full genome. If these three targets are found, how confident can we be that the other 99.3% of the genome needed to be an infectious viral particle is also present?
Apparently, not very.
The Center for Evidence-Based Medicine at Oxford University recently reviewed the evidence that a positive PCR test correlates to presence of infectious virus in the individual testing positive. Their conclusion was not encouraging:
"These studies provided limited data of variable quality that PCR results per se are unlikely to predict viral culture [i.e. infectious particles] from human samples. Insufficient attention may have been paid how PCR results relate to disease. The relation with infectiousness is unclear and more data are needed on this."
A more recent study confirmed the lack of correlation between infectious viral particles and PCR positivity. The study was to determine the extent to which ultraviolet irradiation of infectious viral particles impaired their ability to infect cells. Infectious viral particles of a known quantity were irradiated for different lengths of time. After each exposure two tests where run on those viral particles: one was a direct measure of how many infectious particles remained. The second was PCR to quantify how many "targets" were found in the sample.
Table 1 from that article has the telling data:
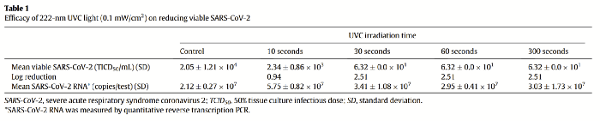
The top row shows the number of infectious particles before ("Control") and after each exposure interval. The number dropped from about 20,000 before exposure to its bottom level of about 60 infectious particles after 30 seconds and beyond. UV light clearly drops viral infectiousness dramatically.
It is the bottom row that tells the tale. Not only did the "viral load" fail to decline as infectious particles fell to very low levels, but the viral copies identified by PCR actually increased somewhat. While the control sample was found by PCR to have about 21 million copies of the target DNA, after 300 seconds of UV exposure that same sample was found to have about 30 million copies. Curiously, after the initial 10 seconds of exposure PCR returned a count of over 57 million copies. It is not that there is poor correlation between infectious viral particles and PCR positivity. It is that there is no correlation at all.
Back to "New Cases"
In spite of the fact that PCR doesn't reflect either the quantity or even the mere presence of infectious viral particles, it is currently the "gold standard" for diagnosis of a case of Covid-19. All other tests that are developed -- antibody, rapid antigen, etc. -- are validated against PCR. This is like grading exams using a key with an unknown number of mistakes on it. This problem has been recognized for several months.
The result of using PCR as the primary diagnostic test is to inflate the number of cases. We are diagnosing an infection with a test that can't determine an infection and, based upon the evidence available, correlates somewhere between poorly and not at all with infectious virus.
The health authorities who have instituted PCR diagnostic testing via the Emergency Use Authorization (EUA) certainly would have been aware of the potential problems with using PCR as a diagnostic test.
On February 3, 2020, CDC submitted an EUA package to expedite FDA-permitted use of the CDC diagnostic panel in the United States. FDA issued the EUA the next day, and CDC sent the test kits to state and local public health laboratories.
With data at hand, they certainly now know that the problems reviewed here have become manifest. Using PCR diagnostically will overestimate by some unknown percent the truly infected people. What about that significant percentage of people, estimated to be around 35%, who test positive but manifest no symptoms? Perhaps they have no symptoms because they have no infectious particles in their body. Perhaps they have that 0.7% of viral DNA, but little or none of the rest, or the rest is chopped up into benign pieces. This would include healthy people who have encountered the virus, their immune system did what it is supposed to do and broke it up into non-infectious fragments to be eliminated. But PCR registers those fragments as a positive test and they become a "new case" statistic.
A very recent hypothesis article suggests that the reason for the increasing discrepancy between diagnosed cases (i.e. PCR-positivity) and the morbidity/mortality rate of the disease may have to do with the very issue being raised here. The authors coin a term for these viral fragments, snippets of viral DNA that include, but are not limited to, the fragments detected and amplified by PCR. They call them SARS-CoV-2 associated molecular particle patterns, or SAMPPs.
Exposure to SAMPPs through contact with them on surfaces, in air particles, and elsewhere leads to immune activation. This can take the form of both antibody formation and T-cell activation. Perhaps it is our exposure to ambient SAMPPs that is furthering development of herd immunity.
"If the existence of SAMPPs mediated immunity in a host is proved with appropriate experimentations, then it will sabotage the need for the expensive RNA/DNA based vaccines."
Why continue with a diagnostic test that can't diagnose an infection but will overestimate case numbers? It's all about perception. The Allies needed to control the behavior of the Germans to execute a successful invasion. With Covid-19 "cases," it is the general public that needs to be controlled. Using PCR to diagnose new cases keeps a constant supply of "ruperts" in the mix, people who are PCR positive (a "new case") but without infectious virus. Control happens through fear, and fear is maintained by the dual ‘body counts' of cumulative deaths and new cases.
Even while new case clusters and hotspots and epicenters and outbreaks continue to flash across headlines daily, the rate of hospitalizations in the US due to Covid-19 -- a much better gauge of the actual human morbidity toll of the disease -- continues to drop. The CDC's data is clear about this, the graph here being overall hospitalization rate.
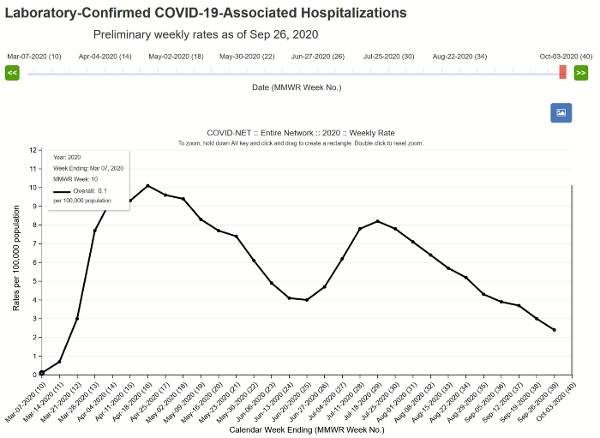
All ages
Announcing that the total disease burden of Covid-19 is dropping in the US is not a provocative way to maintain policies around social distancing, masking, school closures, or other elements of "disease-controlling" social mandates. It is a way, though, to maintain high anticipation for a vaccine, acceptance of contact tracing, an openness to biometric surveillance, and a general fixation on the recommendations of health authorities. Fauci himself is now straddling that line between telling us the economy is ready to open, and reminding us that we must follow this new set of social mandates.
"Don't interpret it as an obstacle to opening the economy," he continued. "Because if you do things the way we have prescribed, namely, a gateway of phase one, phase two, phase three, without jumping over these benchmarks that you have to look for, you can safely get people back to work, get the economy going.
In other words, keep your mask on, keep your distance, and wait with anticipation for the vaccine.
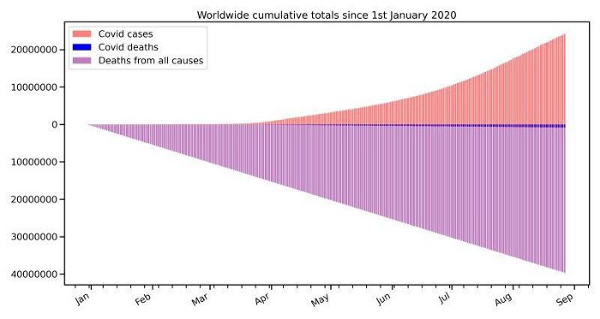
Source: https://swprs.org/covid-the-big-picture-in-7-charts/
The worldwide gulf between cases and deaths is dramatic and widening every day. Once it is understood that a "case" is not necessarily -- and perhaps not even probably -- a case of active infection, there is actually some solace to be found in these high case numbers. They very well might indicate exposures successfully fended off, with T-cells activated and/or antibodies formed.
In other words, many of those new cases might indicate people adding to the pool of herd immunity.